
Thursday evening, Newark Wayne Community Hospital welcomed EMS providers to its new emergency department, which will be opening next month. Dr. Jamie Syrett presented on two topics. The first was resuscitation of the neonate and the pregnant female. Points of interest included:
- Neonatal resuscitation:
- Transition away from APGAR scores to a classification of normal/purely cyanotic (presenting with central cyanosis after 10 minutes)/critical (apneic or HR<60).
- The lack of necessity to suction meconium if the neonate is lively.
- Emphasis on the importance of respiratory etiology of arrest or failure to thrive, with warmth as a close second priority.
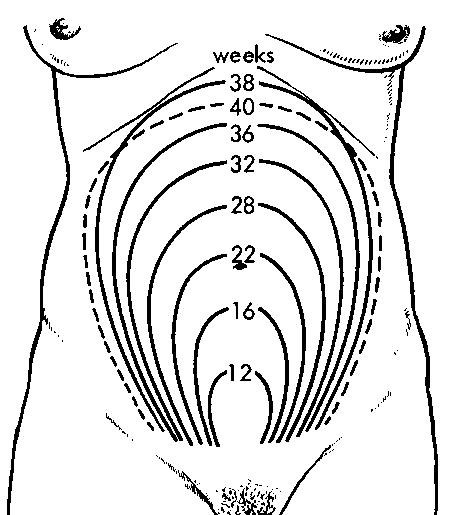
- 22 weeks was given as the guideline for a viable preterm infant. Conveniently, this gestational age corresponds to a fundal height level with the umbilicus or higher.
 OB resuscitation:
OB resuscitation:
- CPR is most effective with a wedge beneath the patient, tilting her 27-30 degrees to the left to relieve fetal pressure on the great vessels. An inverted chair can be used as an improvised wedge to achieve this angle. Failing this, the fetus can be manually shifted by pushing or pulling it to the patient’s left.
- The most effective treatment for the pregnant female in cardiac arrest is removal of the fetus. C-section also potentiates internal cardiac massage via an incision in the diaphragm. These treatments are impractical in the prehospital and even MICU environment and necessitate rapid transport to an appropriate facility.
Dr. Syrett also presented on the topic of driver resuscitation. His guidelines for the aggressive treatment of the crash victim have now been accepted by NASCAR as the nationwide standard of care. This approach brings principles of tactical and wilderness medicine to the treatment of the entrapped driver. Although this protocol was developed for specialized application in formula one racing, many of the principles apply to the treatment of trapped patients in critical condition. The guiding principle of the protocol is to rapidly treat a patient who is suffering life threatening injuries in an austere environment that precludes a complete physical exam. Highlights of the protocol include:
- Placement of CAT tourniquets on all four extremities and application of direct pressure to any other exsanguinating hemorrhage. While not mentioned specifically by Dr. Syrett, hemostatic agents are of course applicable here.
- Rapid establishment of an airway via cricothyroidotomy. The drip chamber of a 60 drip set is cut off and the spike used to improvise a one-step cric. A bag valve mask can be directly attached to the chamber, and ventilation can be effectively established by these means.

- Bilateral needle thracentesis and sealing of any open chest defects.
- Placement of a humeral IO in the accessible shoulder. This access is used for the administration of tranexamic acid to promote clotting and vasopressin to shunt blood away from the abdominal organs.
- As the patient is extricated, the pelvis is bound with either a specialized device such as a t-pod, or a KED which is inverted so the straps wrap around the pelvis. The patient may then be moved to a long backboard.
It is refreshing to see the principles of tactical medicine and aggressive trauma care applied in the civilian prehospital setting, and Dr Syrett’s presentation of these principles to EMS providers at all levels is greatly appreciated. We will provide links to the complete protocol when available.

1 thought on “Dr. Jamie Syrett on neonatal and OB resuscitation, driver resuscitation.”