
by Jamie Syrett, MD, FACEP.
Every year in EMS we see things that we used to do for patients be pushed aside by new data that suggests what we did, actually had no impact on patient care or even worse harmed the patient. Recently we have seen MAST trousers, atropine, Lasix and even cervical collars and backboards get rejected as appropriate care options, but could the same happen with oxygen? Oxygen, come on, really? Well brace yourself, because oxygen is bad for your patient.
Standard EMS management in almost every condition has been to apply oxygen to the patient. Whether it was respiratory distress, major trauma, chest pain or stroke, you got oxygen. In NY at the BLS level you got 2L NC or 100% NRB. With the thousands of hours of additional training ALS providers could even titrate the 2L NC to 4! When EMS arrived on scene and found a patient with an oxygen saturation of 70%, everything was done to increase that number (although the evidence that is beneficial is lacking). Recently some of my friends climbed Mount Kilimanjaro, the highest mountain in Africa. As true EMS geeks they brought a saturation monitor with them. At the top of the mountain their respective saturations were 41%, 73% and 84%, no ambulance needed! So, I think the tide has changed and oxygen is quickly becoming the overused detrimental medical intervention that some of us have always suspected. Lets look at some recent evidence…
In an observational study by Gries RE et al (Chest 1996; 110: 1489-92.) They found that healthy subjects in all age groups routinely desaturate to an average nadir of 90.4% during the night. Conclusion – routine desaturations are common.
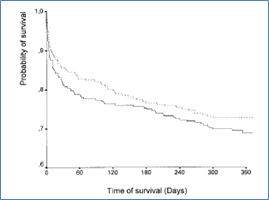
In a study by Ronning OM, Guldvog B. (Should Stroke Victims Routinely Receive Supplemental Oxygen? A Quasi-Randomized Controlled Trial. Stroke. 1999;30:2033-2037) they found that minor or moderate stroke victims did worse when given 100% oxygen. Below are some of their results giving the probability of survival if you are given 100% oxygen versus not. (If you got oxygen you did worse):
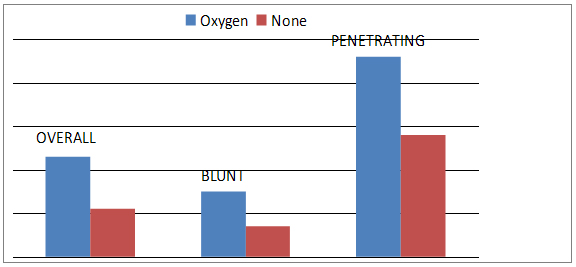
In a study by Stockinger ZT, McSwain NE. (Prehospital Supplemental Oxygen in Trauma Patients: Its Efficacy and Implications for Military Medical Care. Mil Med. 2004;169:609-612) in trauma patients, they found that there was no benefit to giving oxygen to trauma patients unless they required intubation. (5549 patients). Again patients getting oxygen had a higher mortality. (Mortality results below):
Even the dreaded oxygen and COPD patients argument has resurfaced, traditionally EMS were taught that in the short term management by EMS of COPD patients, high flow oxygen was appropriate to use…step in Michael Austin who published in the BMJ in 2010. (BMJ 2010;341:c5462). He concluded that “titrated oxygen treatment significantly reduced mortality, hypercapnia, and respiratory acidosis compared with high flow oxygen in acute exacerbations of chronic obstructive pulmonary disease. These results provide strong evidence to recommend the routine use of titrated oxygen treatment in patients with breathlessness and a history or clinical likelihood of chronic obstructive pulmonary disease in the prehospital setting.” What did that look like in his study… titrated O2 reduced mortality in his study by 58% in all patients and 78% in COPD patients when compared to the 100% NRB.
Finally the thing we have been doing so good on over the last years…Acute MI. Lets take a look at McNulty PH, et al. (Effects of supplemental oxygen administration on coronary blood flow in patients undergoing cardiac catheterization. Am J Physiol Heart Circ Physiol. 2005; 288: H1057-H1062). They demonstrated that within 5 minutes of 100% NRB coronary resistance increased 40% and coronary blood flow dropped 30%. Want to see it…
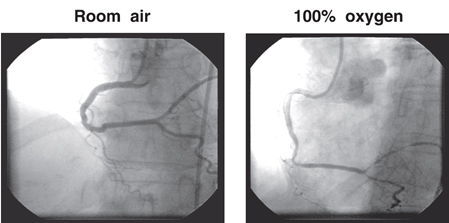
and the flow in the coronary artery…

So in conclusion what does this mean? I suspect that over the next few years in EMS we will see a de-emphasis of oxygen management. Titrating oxygen to maintain saturations over 88% seems like a reasonable goal, and seeing saturations in the low 80s may actually be acceptable. Venturi devices will probably make a return as well. CPAP and nebs may be given using air rather than oxygen and finally the BLS grab bag will not contain the anchor/patient sedation device/oxygen tank!
Thanks to Sam Tinelli and James Rooker who run this site to allow me to write what I hope is a thought-provoking summary. Controversial – Yes, so don’t break your protocols just yet, but get prepared for the change that is coming!
Jamie Syrett, MD, FACEP.
Dr. Syrett is a medical control physician in the Finger Lakes EMS region, and serves as medical director for the Specialty Care Transport program out of Newark-Wayne Community Hospital.
